
Is a Lip Tie Causing Your Nursing Pain? Hidden Signs to Look For
Hello, sweet new parent. Take a deep breath. I know you’re here because something doesn’t feel right. You were told breastfeeding is natural, but for you, it’s been filled with toe-curling pain, frustration, and maybe even some tears. You’re doing everything ‘right,’ but it still hurts. I want you to hear this first: You are doing an amazing job, and your feelings are completely valid.
For over two decades as a pediatric nurse and lactation consultant, I’ve sat with countless parents just like you. And one of the most common, yet frequently missed, culprits behind these struggles is a restrictive labial frenulum, more commonly known as a lip tie. It’s a tiny piece of tissue that can cause a world of trouble for both you and your little one. But here’s the good news: identifying it is the first step toward a solution. Together, we’re going to gently explore the hidden signs, understand what’s really going on, and map out a clear path to get you the support you deserve. Let’s begin.
What Exactly is a Lip Tie? (And Why It Matters for Breastfeeding)
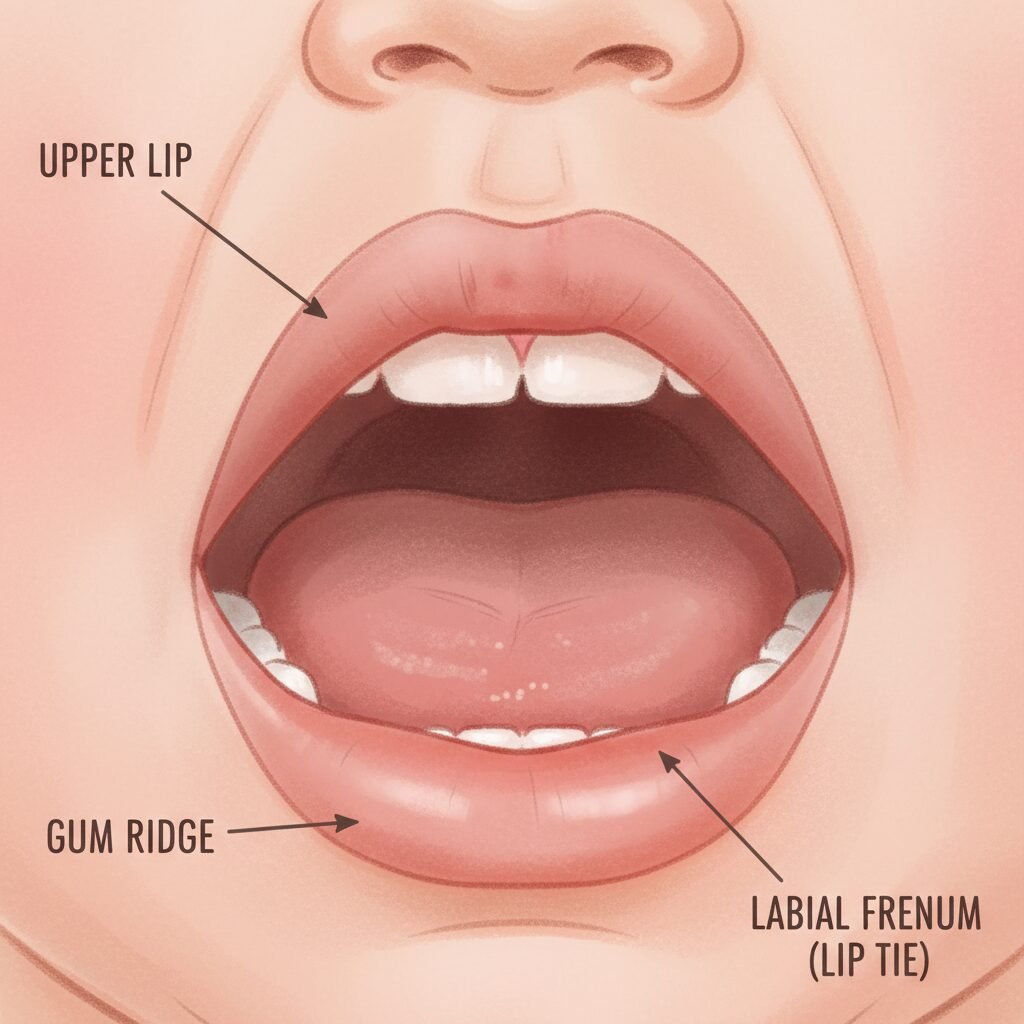
Let’s start with the basics, without any confusing medical jargon. Everyone has a piece of tissue that connects their upper lip to their upper gum. This is called the labial frenulum. In some babies, this tissue is unusually short, thick, or tight. When it restricts the movement of the upper lip, we call it a ‘lip tie.’
Now, why does this little piece of skin matter so much? Picture your baby trying to breastfeed. To get a deep, effective latch, they need to open their mouth wide (like a baby bird!) and flange their top lip outward, creating a good seal around the areola. A restrictive lip tie can make this simple-sounding motion nearly impossible. It tethers the lip down, preventing it from flanging out properly. This leads to what we call a ‘shallow latch.’
Instead of drawing your breast tissue deep into their mouth, your baby may end up just chomping on the nipple itself. This is not only incredibly painful for you, but it’s also an inefficient way for your baby to get milk. They have to work much harder for less reward, which can lead to a whole cascade of other issues we’ll talk about soon. It’s not just about pain; it’s about the fundamental mechanics of feeding. Understanding this connection is the key to figuring out your next steps.
A Gentle Reminder: The presence of a visible frenulum is normal! A ‘tie’ is only a problem if it’s causing a problem. We focus on function, not just appearance.
Hidden Signs in Mom: More Than Just Nipple Pain

You are the first and most important indicator that something might be off. Your body is giving you signals, and it’s crucial to listen to them. While nipple pain is the most obvious sign, the clues often go much deeper. See if any of these sound familiar:
- Misshapen Nipples Post-Feeding: After your baby unlatches, take a look. Does your nipple look creased, flattened, or shaped like a brand-new tube of lipstick? This is a classic sign of a shallow latch, where the baby is compressing the nipple instead of drawing it out.
- Cracked, Blistered, or Bleeding Nipples: While some initial tenderness is common, breastfeeding should not cause continuous damage. Persistent cracks, blisters (vasospasms), or bleeding that doesn’t heal are major red flags that the latch mechanics are wrong.
- A Feeling of Being ‘Used as a Pacifier’: Does it feel like your baby is constantly nursing but never seems satisfied? This can happen when they can’t effectively drain the breast, so they nurse for comfort and for long periods just to get enough milk.
- Recurrent Plugged Ducts or Mastitis: When milk isn’t removed efficiently from the breast, it can back up, leading to painful plugged ducts or a full-blown breast infection (mastitis). If you’re getting these repeatedly, it’s often a sign of poor milk drainage, which can be linked to a poor latch from a lip tie.
- A Drop in Milk Supply: Your milk supply is based on demand. If your baby can’t effectively stimulate and empty the breast, your body might get the signal to produce less milk over time.
If you’re nodding your head to several of these, please know that this is not your fault. It’s not a reflection of your ability to breastfeed. It’s simply a sign that there’s a physical barrier we need to investigate.
Telltale Signs in Your Baby: What to Look For

Your little one is giving you clues, too, though they can be a bit more subtle. A baby with a restrictive lip tie is often working overtime to eat, and this effort shows up in various ways. Let’s decode your baby’s signals:
- A Clicking or Smacking Sound While Nursing: This sound often indicates that your baby is losing suction. Because their lip can’t maintain a good seal, they may repeatedly break and re-establish suction, making that telltale ‘click.’
- Poor Weight Gain or Slow Weight Gain: This is a big one. If your baby is struggling to gain weight despite nursing around the clock, it’s a strong indicator that they are not transferring milk effectively.
- Excessive Gassiness, Fussiness, or Reflux Symptoms: A poor seal means the baby is often swallowing a lot of air along with milk. This can lead to a very gassy, uncomfortable, and fussy baby. Sometimes, this is misdiagnosed as colic or reflux.
- Falling Asleep Quickly at the Breast: Is your baby nursing for a few minutes and then immediately falling into a deep sleep, only to wake up starving 30 minutes later? This is often due to exhaustion. They are working so hard to get milk with a poor latch that they tire out before they can get a full feeding.
- A Sucking Blister on the Upper Lip: You might notice a little callus or blister in the center of your baby’s top lip. This forms from the friction of their lip rubbing against the breast because it can’t flange out properly.
- Inability to Hold a Pacifier or Bottle Teat: The same mechanics apply here. A baby with a lip tie might struggle to create and maintain the suction needed to hold onto a pacifier or bottle teat effectively.
Remember, your baby isn’t being ‘difficult.’ They are doing the best they can with the anatomy they have. These signs are their way of communicating that they need a little help.
Is It a Tie or a Normal Lip? A Quick Visual Guide

Okay, so you’re probably tempted to gently lift your baby’s lip right now. That’s a great instinct! But it can be confusing to know what you’re looking at. A visible frenulum is present in all babies; the key is whether it’s restrictive. Let’s break down what to look for, but please remember, this is not a substitute for a professional evaluation.
Gently lift your baby’s upper lip towards their nose while they are calm and relaxed. What do you see and feel?
| Characteristic | Normal Upper Frenulum | Potentially Restrictive Lip Tie |
|---|---|---|
| Appearance of Lip | The upper lip flanges out easily, looking full and relaxed. | The upper lip looks thin or tight and may have a hard time flanging out. It might even look like it’s being pulled inward. |
| Where It Attaches | The tissue attaches high up on the gum line, well above the future tooth line. | The tissue attaches low on the gum ridge, sometimes wrapping through to the hard palate. |
| Flexibility | The tissue is thin, stretchy, and elastic. You can easily lift the lip. | The tissue is thick, tight, or rigid. You meet significant resistance when trying to lift the lip. |
| Effect on Lip Shape | When you lift the lip, it forms a gentle, wide arc. | When you lift the lip, you may see blanching (the gum tissue turns white from the tension) or the lip may form a heart shape. |
Safety First: Never force your baby’s lip or mouth. A proper assessment should be done by a trained professional, like an IBCLC (International Board Certified Lactation Consultant) or a pediatric dentist/ENT who specializes in tethered oral tissues.
This table is a guide to help you gather information, not to self-diagnose. Your observations are valuable data points to share with a provider who can look at the full picture of your baby’s oral function.
You Suspect a Lip Tie… Now What? Your Action Plan

If this article is resonating with you, your head is probably spinning with ‘what ifs’ and ‘what nows.’ It’s okay. Let’s turn that anxiety into action. Here is a clear, step-by-step plan to get the answers and help you need.
- Book an Appointment with an IBCLC. This is your most important first step. An IBCLC is a lactation specialist who can perform a full functional assessment. They will watch a feeding, assess your baby’s oral anatomy, and help determine if a lip tie (or tongue tie, which often accompanies it) is impacting function. They can also provide immediate help with positioning and latch to give you some relief.
- Assemble Your ‘Care Team.’ Based on the IBCLC’s assessment, you may be referred to other providers. The best teams often include a pediatric dentist or an Ear, Nose, and Throat (ENT) doctor who specializes in releasing oral ties. It’s crucial to find someone experienced in this specific area. Ask for referrals from your IBCLC or local parenting groups.
- Discuss Treatment Options. If a restrictive tie is diagnosed, the treatment is a simple in-office procedure called a frenectomy. This is where the tight tissue is released, usually with a sterile scissor or a laser. Your provider will walk you through the entire process, including pain management for your baby (it’s very minimal and brief) and what to expect.
- Commit to Aftercare. Releasing the tie is only half the battle. The tissue will want to heal back together. Your provider will give you a series of simple stretches and exercises to perform on your baby’s lip for a few weeks post-procedure. This aftercare is critical to the success of the revision. It ensures the lip maintains its new, free range of motion.
- Follow Up with Your IBCLC. After the procedure, your baby has to learn how to use their newly freed lip! It’s a whole new world for them. A follow-up visit with your lactation consultant is essential to help your baby re-learn how to latch and breastfeed effectively and pain-free.
Navigating this process can feel overwhelming, but you don’t have to do it alone. Building the right support team is everything.
Conclusion
My dear parent, if you’ve made it this far, I hope you feel seen, heard, and most of all, empowered. The pain and frustration you’ve been experiencing are real, but they don’t have to be your entire breastfeeding story. Whether the issue turns out to be a lip tie or something else, trusting your instincts and seeking answers is the most powerful thing you can do for yourself and your baby.
Remember, breastfeeding is a relationship, not a performance. It has ups and downs, and it’s okay to ask for help. You are your baby’s greatest advocate. By investigating these hidden signs, you are already taking a massive step toward a more comfortable, joyful, and sustainable feeding journey. Be gentle with yourself, gather your support team, and know that there are solutions out there. You’ve got this.





